While the summaries of the hepatitis B vaccines are not that long, their mistakes are so extensive, and their efforts at deception so persistent, that this will be a long blog post. The format of this post will be in quote and response.
Common side effects of the hepatitis B vaccine include fever, diarrhea, and fatigue/weakness.
While this sentence by itself is reasonably accurate, they forget the most common side effect, which is transient pain at the injection site or nothing at all. They use the common antivax tactic of setting up subtle distortions to help the reader accept their more outrageous distortions later in the article.
A more serious potential side effect is seizure, which may occur in about 1 in 1,300 children vaccinated with the hepatitis B vaccine.
They make multiple errors and inconsistencies in this sentence – for example, citation #6, the Institute of Medicine report from 2012, explicitly states that while there have been seizures reported after the hepatitis B vaccine, there is no evidence to link those seizures to the hepatitis B vaccine itself. The PIC group is citing evidence only when it suits their point of view, and de-emphasizing the parts that would put holes in their narrative. Again – informed consent is only informed when the information is presented holistically and in the correct context. Next, they try to pass off the rate of seizures as 1/1300 through making really serious statistical errors that would normally be caught in high school. They try to compare the rate of seizures after measles to the rate of seizures after the hepatitis B vaccine, by looking at the absolute number of reports sent to VAERS. The number of reported seizures after the hepatitis B vaccine was 437 from 1993-1997, when the number of reported seizures after the MMR vaccine was 940. The PIC group forgot to thoughtfully calculate the denominator! It is primary school mathematics, to realize that 940 is not necessarily bigger than 437 if the denominators are wildly different. Specifically, 940/1000 is bigger than 437/1000, but 940/6 000 000 is smaller than 437/1 000 000 . Again, their own citation #6 does not find a significant link between hepatitis B vaccine and seizures. If PIC were genuinely wanting to make vaccines better, they would try and investigate those rare children who have seizures and figure out what genetic changes might predispose them to seizures. They don’t really put their money where their mouth is, though.
Although serious side effects have been observed following hepatitis B vaccine, including neurological disorders…
The correct thing to do with such a hypothesis is to convene a committee and examine the evidence, or start epidemiological experiments to make new evidence. One such committee specifically determined that the evidence rejects an association between the hepatitis B vaccine and multiple sclerosis. In fact, more modern research has found that the cause of most multiple sclerosis is Ebstein-Barr virus. There are other papers that have looked specifically at seizures and demyelinating diseases, and they find no link. A seizure may look scary to the family experiencing it, but the seizures occur in such tiny numbers that the evidence points towards no link.
For children, the hepatitis B vaccine contains 250 mcg of aluminum. This amount is 75 times greater than the maximum safe level of aluminum in the bloodstream per day for a 7.3-pound (3.3-kilogram) infant, derived from the Agency for Toxic Substances and Disease Registry (ATSDR), a division of the U.S. Department of Health and Human Services (HHS) (Fig. 1).
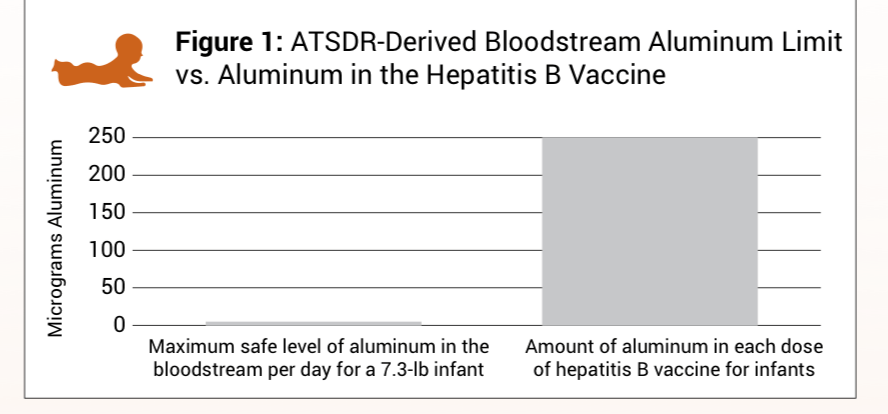
The quote and its accompanying figure above make really fundamental mistakes in biology. The most fundamental mistake is to mix up blood stream concentration and vaccine concentrations. If a vaccine is given correctly, it is not being given directly into the bloodstream of a person. This comparison, is therefore, meaningless. A real life analogy would be to complain about someone getting water toxicity if they attempted to drink an entire water truck full of water, when we all know that humans drink small servings of water at a time. For a description of aluminium as it is relevant to vaccines by someone who actually understands the blood-brain barrier, see here.
How accurate is surveillance of side effects from the hepatitis B vaccine?
The paragraph that follows this sentence is so terrible that it contradicts itself. At the beginning of the sentence, they want the reader to believe that there were 114 deaths or permanent disability after hepatitis B vaccine as recorded by VAERS from 1993-1997, however, at the end of the paragraph the authors complain that VAERS does not provide an accurate count of hepatitis B vaccine side effects. If PIC actually cared about investigating these deaths, they would actually investigate what caused them, which these particular investigators did. They noted that the kids in question died of bacterial pneumonia and asphyxiation by foreign body in most cases, which has no plausible connection to the vaccines. PIC mainly wants the amount of side effects to be as high as possible so they can sell more fear.
Prelicensure trials usually do not have the ability to detect rare adverse events or adverse events with delayed onset.
This sentence engages in deception by omission of key facts, which is PIC’s favorite tactic. While it may seem that “big pharma” has unlimited financial resources, they actually do not. PIC is calling for massive clinical trials without thinking about the amount of funding or logistical coordination that such trials would require. Even a company as financially well off as a pharmaceutical company must “draw a line in the sand” as to how many people they can enroll for a clinical trial. In reality, there are multiple clinical studies that occur after the initial licensure trials (post-marketing) that are intended to look for rare side effects. Making this kind of claim is similar to complaining that a car company failed to notice an issue resulting in a recall. Most car companies do their pre-release testing as diligently as possible, but sometimes the engineering team didn’t anticipate a specific real-world condition that would result in a condition requiring a recall. That requires real-world testing with real customers after the car is released. One only has to view Pubmed to see over 12 000 papers pertinent to the hepatitis B vaccine to see how much safety research has been done on it.

The graph illustrating the larger potential risk of permanent injury from the hepatitis B vaccine is like a Russian matryoshka doll of deceptive statements. I had to find 3 nested citations to dig up where this study came from, but this is the actual paper that this graph was derived from. The first layer of deception is that the PIC authors failed to disclose the title of the paper – no increase in demyelinating diseases after hepatitis B vaccination. The next level of deception is how they labeled the right bar as “potential risk of permanent injury”, when the study was clearly looking at demyelinating diseases. Thirdly, we now know the cause of multiple sclerosis – it is Ebstein-Barr virus, so discussion about hepatitis B and its relationship to multiple sclerosis should cease. Lastly, the confidence ratio touted by the PIC authors is 0.4-2.1, which includes 1 – that means there was no significantly increased risk according to the study results. In plain words, that means that within the ability of the study to measure, there was no significantly increased risk of demyelinating events in the vaccinated versus unvaccinated control groups. Besides, a large group of demyelinating diseases in children are known to be caused by other viruses like enterovirus. So, yet again, there is absolutely nothing of substance in this graph.
Infants and children usually don’t experience any symptoms of hepatitis B, and about 50% of adults don’t experience any symptoms.
This sentence is deception by omission. While it is true that most kids feel minimal to no symptoms, what they don’t tell you is the proportion of kids who go on to become adults with chronic infection, liver malfunction, and liver cancer. Because hepatitis B as of 2024 carries no cure, the risk of these conditions is significant. 15-40% of people who are chronically infected with hepatitis B go on to develop those serious complications. The antivaxxers don’t care about that.
Hepatitis B is spread through the mixing of bodily fluids with those of an infected individual, usually involving infected blood. In the United States, the most common
routes of transmission are by sexual contact among heterosexuals with multiple partners or men who have sex with men, and injection drug use.2 The virus can also be transmitted by being born to an infected mother.2 Casual contact with an infected individual’s saliva, tears, sweat, and urine are unlikely modes of transmission.2 Hepatitis B is not transmitted by breastfeeding, kissing, hugging, holding hands, coughing, sneezing, or sharing dishes, eating utensils, or drinking glasses.
While this paragraph is correct in broad strokes, it is strategically placed to help the fan of PIC to minimize the possibility of transmission to infants and children, and therefore encourage the parent to refuse pediatric hepatitis B vaccination. It is also highly false that kids can only get the virus through IV drug use – kids most commonly contract hepatitis B through casual activities like a family member unknowingly bringing the virus in through a kiss on the cheek, or accidentally using a shared toothbrush. The highest degree of vaccine hesitancy for the hepatitis B vaccine exists against the birth dose of the hepatitis B vaccine, but although the United States is relatively unique in offering this dose, there is an epidemiologic reason. While the childhood hepatitis B vaccines were introduced, they were not effective in driving down the infection rates of infants. This meant that there was still community transmission – hence the reason to add the dose of hepatitis B vaccine at birth (citation GAVI). In addition, PIC and people who think like them love to omit that the hepatitis B virus is very hardy, and can live on inanimate objects for around seven days. Because hepatitis B vaccine has no cure, and contact between broken skin and an infected surface can set up an infection in an infant, hepatitis B vaccination at birth provides additional protection. Quite a few parents refuse the birth dose of hepatitis B because it is perceived as a criticism against the mother. However, offering this vaccine is genuinely not meant as an insult as some families may perceive them – to offer perfect shielding against hepatitis B would mean that the mother has to test negative for this infection and also shield the child from every possible inanimate object that could contain this virus.
Prior to 1991, before widespread use of the hepatitis B vaccine began, hepatitis B was a disease of low incidence… Despite widespread use of the hepatitis B vaccine for more than 25 years, the prevalence of chronic hepatitis B infection in the U.S. has remained about the same since 1976, when the rate was 0.3% of the population.9 It is estimated that between 1 in 60,000 (0.0017%) and 1 in 80,000 (0.0013%) individuals die annually from hepatitis B-related liver cirrhosis or liver cancer.
The PIC group almost understands the seriousness of hepatitis B! Well done! However, they fail at understanding that before patients get to cirrhosis or liver cancer, they have to deal with many years, sometimes decades, of impaired lifestyle, suffering, and disease. Hepatitis B vaccine prevents that. This data also refutes the figure illustrating the annual risk of contracting a fatal hepatitis B infection for a kid – it’s not the eventual possible death that is the first priority to avoid, it is the illness, suffering, and disease as well.
Because hepatitis B resolves on its own in most cases, usually only supportive treatment is necessary.
This is a false statement because they are referring to adults, who genuinely can clear a first time infection most of the time if they are immunocompetent, but the kids are the population that are really relevant in this discussion.
The crux of the logical mistake is – in order to become an adult, an adult must first be a kid.
The younger the child, the more likely they are to set up a chronic infection. The more chronic infections you have, the more children go on to develop cirrhosis. Remember even in adults, if the majority of people clear the infection, there is still a few percent of adults who get chronically infected. A few percent spread across the entire US adult population is a large number of adults. The other problem with this argument is that many of the medicines mentioned have considerable side effects, which is something the PIC group has been railing against! At this point we can discern that side effects matter for injectable items, but they don’t matter for pills to PIC. The cognitive dissonance is on full display. The vaccination is still the simplest way to get protection. What’s the solution for waning protection? Boosters are available. Some patients with prior liver conditions for example, stand to benefit the most from vaccine boosting for hepatitis B.
The vaccine has not made a measurable impact on the prevalence of chronic hepatitis B.
This statistic lies by deception – the hepatitis B vaccination when given in neonates decreases the amount of chronic hepatitis B infection in neonates by around 90%, and is most effective in maximizing the effectiveness of the hepatitis B series in countries where hepatitis B prevalence is high. Another way to look at this is to observe that there were 18 000 children under 10 who contracted new hepatitis B infections before there was a newborn hepatitis B vaccine (and just the 2,4,6 month doses). While hepatitis B’s initial symptoms may be subtle, its consequences as an adult are not at all subtle – which is why vaccination is worth the time and effort.

Leave a comment