Ron Johnson recently invited Peter Mccullough, Joel Wallskog, James Thorp, Jordan Vaughn, Aaron Siri, and HI governor Josh Green to testify about COVID vaccine myocarditis on May 21 2025. While a handful of themes were reasonable, most of the testimony repeated many of the same lies and misrepresentations that these characters have used again and again throughout the last five years. This article aims to explain the most significant mistakes in the testimony. If you have been reading my prior writing, you’ll see that many of the points I made previously about these speakers still remain true. An overwhelming theme of this testimony is for the main characters to spew as much information as possible so that very few people are capable of fact checking them in realtime. In contrast to prior hearings by Johnson, dissenting voices like Senator Blumenthal were allowed in to counter his views.
The most serious problem with this committee is that they are spending so much time on COVID myocarditis when they really should be putting out a clear message about emerging infectious diseases like measles. The boss of the HHS is going out and only with extensive arm twisting, can he finally say that people should get vaccinated against measles. He is still looking for ways to spread an antivaccine message via creating sufficient doubt. Worse still, it is the policy of the current government to extensively cut funding to multiple public health agencies so that they cannot warn the public as effectively for the next significant infectious diseases. Given that this debunk is so long, I will provide links that jump to the relevant segment of this page so the interested reader can jump around if desired. Press the home key to jump back up to the top to get to this table of contents.
Allegation – there were so many more adverse events reported.
Allegation – there was insufficient attention paid to early treatment.
Allegation – the CDC failed to warn the American public about the COVID vaccine myocarditis risk.
Allegation – COVID vaccines decrease fertility.
Allegation – COVID vaccine myocarditis is severe.
Allegation – so many people died due to the COVID vaccine.
Allegation – they lied about the COVID vaccine staying in the shoulder.
Allegation – there is a 82% miscarriage rate in COVID vaccines.
Allegation – you can’t sue vaccine companies.
Allegation – the immunization schedule has expanded too much.
Allegation – the vaccine companies spent too little time doing the randomized controlled trials.
Allegation – Peter Mccullough is one of the most published [researcher on COVID].
Allegation – there were 216 COVID vaccine deaths in 2025.
Allegation – all vials of the vaccine are not the same.
Allegation – clotting issues affect what we are seeing in the vaccine injured and long COVID.
Allegation – “independent researchers with no financial conflicts of interest”
Allegation – “[the vaccines] induce fibrin resistant to breakdown”
Allegation – “neurological events are the most common side effect after the vaccine”.
Allegation – “3 million lives saved due to COVID vaccines came from a blog”.
Allegation – “we had an increase in all cause mortality”
Allegation – “the COVID vaccine hijacks the cell”
Allegation – “mRNA vaccine was designed to be unassailable by the body to be broken down”.
Allegation – “the spike protein is found all over the body”.
Allegation – “Later COVID mutations were intrinsically more mild”
Allegation – “They lied to us about COVID vaccines blocking transmission”
Allegation – “statistically zero kids under 5 died of COVID”
Allegation – “it was a bad idea to close schools”
Allegation – “we’ve seen long white blood clots in autopsy”
Allegation – “ventilators are the worst thing you could have done to people”
Allegation – “they should have designed the vaccine against SARS-COV2 nucleoprotein”
Allegation – COVID vaccine inserts were intentionally left blank
Allegation – it was reckless to not provide advice on how to decrease the risk of cardiac arrest
Allegation – there is a larger group of subclinical myocarditis
Allegation – a study has shown micro scars years after COVID vaccine
Allegation – Vsafe was intentionally designed to not capture adverse events of special interest
Allegation – there were so many more adverse events reported.
While this allegation is true on the surface, you have to also take into account reporting bias. What that means is, not all vaccines had the same amount of interest from the public in reporting side effects. Because COVID vaccines are the most studied vaccines in history and some of the most well covered by the traditional and independent news media, people are naturally going to be inclined to report more issues via the VAERS and V-safe systems. This does not necessarily mean that there are intrinsically more side effects. Although COVID vaccines are known for their ability to generate myocarditis in young men, they aren’t the first vaccine in history to do so. If 15 000 people reported a sore arm after the COVID vaccine as compared to only 4000 in an older vaccine, it still means that COVID vaccines give most people sore arms. The statistic presented by senator Ron Johnson on its own is misleading. The opposite statement is also false – the allegation that VAERS understates adverse reactions. This statement refers to the “Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS)“. We already know that serious reactions are already reported routinely to VAERS and detected, and we also know that despite small numbers, famous vaccine reactions like intussusception were detected and dealt with.
Allegation – there was insufficient attention paid to early treatment.
Early treatment that works is called medicine. Unfortunately, the early treatment that Senator Ron Johnson hangs on to has been repeatedly proven (see IDSA Guidelines on the Treatment and Management of Patients with COVID-19) to be ineffective. The best early treatment is still vaccination and masking.
Allegation – the CDC failed to warn the American public about the COVID vaccine myocarditis risk.
The committee provides the 55 page document as evidence that the CDC failed to adequately warn the public. The first reports of vaccine myocarditis were correctly assessed as coming from the Israeli Ministry of Health in approximately January-February of 2021. Ron Johnson feels the total timeline between CDC notification and warning the public was too long – except that significant known vaccine side effects like intussusception for the old rotavirus vaccine, was assessed by the CDC and published with approximately the same timeline. The CDC cannot assess causality just by copying and pasting another Ministry of Health’s data. They have to assess the data themselves and see if the same problem is occurring in the United States. By April of 2021, the US CDC noticed that the amount of vaccine myocarditis was greater than expected due to random chance, and the CDC’s partner organization, the ACIP, discussed vaccine myocarditis across multiple different meetings (which Ron Johnson has neglected). The emails that he considers to be conspiracy to cover up myocarditis actually illustrate public health staff members debating with each other about how soon to warn and how to carry out the warning. The US CDC took the Israeli MOH’s word seriously from the beginning but just like in a friendship – you should trust but verify. Hindsight is always 20/20 and we can always complain that “they” didn’t work fast enough, but the email assortment on the document clearly illustrates they were working on this. If Senator Ron Johnson actually wanted to help, he would have helped the CDC get more employees hired to work on this. He did not such thing, he just criticized the CDC to score political points.
Allegation – COVID vaccines decrease fertility.
This allegation originated from a person who thought that a protein that lives normally on the human placenta might be similar enough to COVID spike protein that it will cause the immune reaction to destroy the pregnancy. This uses the antivax strategy of twisting a kernel of truth. Many proteins share similar basic building blocks because that structure, over evolutionary time spans, has served its purpose well. While the structures of the two molecules do share similarities, we have multiple pieces of epidemiologic data that refute the allegation. First, pregnancy is a high-risk state in reference to COVID disease, and getting COVID vaccinated has no association with the risk of miscarriage. Second, COVID vaccines have no effect on female or male fertility. Third, while birth rates during the first few years of COVID went up and down, the obstetricians have had no shortage of work to do. Specific birth rate drops have complex multifactorial reasons such as the relative lack of parental support from the government in the US compared to in European countries. It’s not fearmongering to say that COVID vaccines are very important in pregnancy because COVID disease puts mum and baby at risk, it is a well established fact at this point.
Allegation – COVID vaccine myocarditis is severe.
This statement is especially egregious coming from the cardiologist who shared this; he should know better but knows the picture he prefers to paint. First off, myocarditis has several severities which are explicitly spelled out by one of the professional institutions of cardiologists in the United States. The speaker intentionally shared the most serious anecdotes of vaccine myocarditis to generate a more persuasive message. The epidemiology is very clear that while severe cases exist, they are in the minority. Every country that has studied vaccine myocarditis epidemiology has reached the same conclusion, that most vaccine myocarditis is mild. It is exceedingly disingenous of a cardiologist to rely on anecdotes when he has solid epidemiological data, but makes sense when he knows he is in the antivaccine camp. Myocarditis may be subjectively and emotionally severe to the patient, which is a theme throughout this testimony that is legitimate. I agree with the need to put forth your best effort in hearing what a patient has to say. However, patients with myocarditis needing machines to support their heart are clearly in the minority (that would be medically severe myocarditis).
Allegation – so many people died due to the COVID vaccine.
This statement is ignorant of the concept of autopsy. If one day in the future we had instantaneous autopsy by robots, we would not need statistics and speculation on why people die, we would just have the answer. Unfortunately, we have to work with the tools that we have to systematically determine the reason for death, and to respect the family by providing an accurate cause of death. Peter Mccullough’s assertion is that most people who died after COVID vaccine died due to the COVID vaccine/ vaccine myocarditis. Every epidemiological study which has assessed this, shows this assertion is false. Mccullough’s own citations that he references in his paper even show that vaccine myocarditis with severe outcomes is exceedingly rare. Mccullough is on record diagnosing American football player Damar Hamlin with vaccine myocarditis by watching TV, and doubling down even as Mr Hamlin came forth with his actual diagnosis of commotio cordis (a rare heart rhythm problem that occurs with trauma). Mccullough also cites his own article that claims to document many uncounted deaths from the COVID vaccine – except this article was at its core, a personal opinion piece that some people died of vaccine myocarditis with a failure to logically assess other contributory causes. Senator Ron Johnson does actually ask Mccullough to cite evidence – except Mccullough is alert enough to know he can bluff his audience via citing personal opinion pieces that aren’t actually rigorously peer reviewed research. What’s even worse is, the piece that Mccullough cited was retracted during peer review due to severe methodological errors. You can trick people into thinking hundreds of thousands of people died of COVID vaccines if you write an opinion piece saying so, and then cite yourself (pretending to have created peer reviewed literature). Science doesn’t work like that.
Allegation – they lied about the COVID vaccine staying in the shoulder.
This statement tries to get public health staff on the hook for not accurately describing the biodistribution of the COVID vaccine. While I can support the movement to make public health officials accurately describe certainty and less certain data, it is simply wrong to criticize the biodistribution of the COVID vaccine as being intrinsically nefarious. The immune cells have always taken up vaccine pieces into lymph nodes distant from the site of injection and conducted processing. The interpretation about the “Japanese biodistribution study” is a false interpretation both because they used it to scare people about fertility and because the dose used to assess the mice biodistribution far exceeds what any human would take in one vaccine. Antivaxxers have always enjoyed scaring people about the “loss of fertility”; this trope is not unique to the COVID vaccine.
Allegation – there is a 82% miscarriage rate in COVID vaccines.
Buckle up for a long explainer. This comes from a very specific article authored by Shimabukuro et al. Here’s my deep dive into “Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons”.
Short answer – the article has no concerning findings, in fact it speaks to the safety of COVID vaccine in pregnancy. Read on to understand WHY this is the case.
My first move is to quickly look at the affiliations of the authors – Dr Tom Shimabukuro is a member of the ACIP, the American organization that helps the CDC generate the vaccine schedule, and the senior author is Dr Dana Meaney-Delman, who is a board certified obstetrician. Therefore, my first general impression is that this crew is plenty qualified to be speaking on COVID vaccines in pregnancy.
Their goal was to determine the safety during pregnancy, of the new set of COVID vaccines, and they gathered data from the easiest database available – the V-safe and VAERS registries, and picked up 35691 total entries. Ever since the announcement from Michael Yeadon came out that he was suspicious that COVID vaccination should generate placental autoimmunity – the world community is abuzz to try and determine whether or not that assertion is true. Hint hint – his assertion was based upon the assumption that placental syncytin (a placental protein) is similar to the COVID spike protein generated via vaccination. The similarity is only 4 amino acids, and every protein that needs to be buried in a membrane must be buried there using a specialized structure that is essentially the same. Real-life analogy – if you looked at concrete rebar in buildings, its essentially the same no matter what country you look in. Biochemically – the assertion of fertility problems has no biochemical basis whatsoever. Now, this article is one of the many steps to try and show the hard data backing up safety in pregnancy.
Pregnant folks are always excluded from initial clinical trials unless a medication is specifically designed to be used in pregnant folks – this is because of decades of experience of medicines acting differently during pregnancy than outside of pregnancy. Two classic examples of this are thalidomide and lisinopril (and by the way, thalidomide was never approved by the United States FDA). However, testing in pregnant folks is still very necessary for those who are willing to participate, because COVID disease has the potential to hurt pregnant women very badly.
I quote from the study itself next –
Eligible persons are those who received vaccination during pregnancy or in the periconception period (30 days before the last menstrual period through 14 days after) and are 18 years of age or older. For persons who choose to enroll, the pregnancy registry telephone-based survey collects detailed information about the participant, including medical and obstetric history, pregnancy complications, birth outcomes, and contact information for obstetric and pediatric health care providers to obtain medical records; infants are followed through the first 3 months of life.
What outcomes were measured?
- symptoms after mRNA vaccination amongst all folks 16-54 years of age
- When analyzing pregnancy outcomes, they restricted their analysis to completed pregnancies (and are at the time of publication still following some pregnancies which were not completed)
- they also looked at spontaneous abortion/ stillbirth
- they also looked at neonatal outcomes
What were their results?
- 19252 women were pregnant in the Pfizer vaccine group, and 16439 were pregnant in the Moderna group
- most folks were 25-34 years of age; multiple races were represented, including Caucasian, Hispanic, Non-Hispanic White, Asian, Black, multiracial, American Indian/ Alaskan native, Hawaiian/ Pacific Islander, and other
- shoulder pain, fever, headache, and muscle aches were across the board, the most common reported symptoms after vaccination, and these happened more frequently after dose 2
- the percentages of people feeling symptoms are similar to women who weren’t pregnant
Next, they go and further stratify their results, meaning dive deeper into the subgroups that were enrolled from the entire pot of 35691 participants. The people who claim there is an 83% rate of miscarriage made basic mathematical errors based in their biases against vaccination. The authors themselves directly mention, that their entire cohort of patients will be followed to the completion of pregnancy – and that not all surveyed participants had delivered babies by the end of the survey. Brian Tyson, one of the originators of this conspiratorial thinking, is a California-based family medicine physician, and for him to accuse mothers of losing their babies due to “not being careful”, is a brutally insensitive thing to say from someone who should have trained in seeing pregnant women and being sensitive around them.
The science of miscarriage actually has solid historical data showing the majority of miscarriages happen because there is something incompatible with life with the fetus (citation ACOG).
The first group of people analyzed are the main focus of the study, and this comprised 3958 participants of the original > 30 000 identified patients. They called 3958 people who received COVID vaccines during pregnancy and asked what happened with these pregnancies. 712 gave birth to healthy babies, 104 miscarriages happened, and 1 stillbirth happened. The rest were still pregnant by the time of the survey. All 30 000 people didn’t all have babies with the same birthday – you have to work with what you have to start off.
In order to compare miscarriages identified during a brand-new study one must compare to historical data – and the historical data speak of around a 12-18% rate of miscarriage. This excellent citation provides the source for that. The data calculated from the study at hand have an important problem to consider before we can actually calculate the rate of miscarriage from the 3958 participants – because lots of people from the study were still pregnant, not all pregnancies were completed. There are two mathematical options for dealing with this. The way the authors work through this is to calculate the number of miscarriages and compare it to the total number of completed pregnancies. This gives a number of 12.6%, which is similar to historical rates. This is Option #1.
A common counterpoint at this point is to say – OK, many Moms with completed pregnancies received vaccinations in the 3rd trimester, so they should be excluded because miscarriages don’t happen as much in the 3rd trimester. Option #2 is to then look back at the numbers in the paper to calculate the miscarriage rates in the 1st trimester and 2nd trimester separately, which are 96/1132, and 8/1714, which are 8.5% and 0.5% respectively. The authors of the paper decided to tread cautiously and report the higher number (considering the disadvantages of both methods).
The crowd opposed to vaccination during pregnancy will say it’s better to exclude the 700 people vaccinated during the 3rd trimester, making the denominator 127, and the number of miscarriages 104, which makes the scary number of “>82% miscarriages”. This then also assumes that the anti-vaccination crowd genuinely believes that pregnancies are completed within 3 months after the 1st trimester. The only way that can happen is via a miscarriage. So from the data given in the paper so far (for which followup was planned by the authors), the true miscarriage rate is 12.6% amongst the participants in the study. This rate is consistent with previous data. The moral of the story is pregnancies don’t last 3 months in humans.
Allegation – you can’t sue vaccine companies.
Remember they like to say this while RFK Jr and Aaron Siri makes quite a lot of money suing vaccine companies 😉 . Just look at the Informed Consent Action Network to see how many lawsuits are against vaccine companies and their associates. Antivaxxers have previously taken vaccines off the market due to actual or threatened litigation. The current vaccination compensation schemes in the United States were created due to two reasons. The first is to compensate those people legitimately experiencing significant side effects such as intussusception, after the old rotavirus vaccine Rotashield. The second is to shield vaccine companies from actual vexatious litigation initiated by antivaxxers to eliminate vaccine access (see previous link). While a pharmaceutical company may be big compared to an individual, they still have an obligation to make money and will pull products if there is too much dishonest litigation.
Allegation – the immunization schedule has expanded too much.
You can still sue the vaccine companies for side effects but you need to follow the laws of your country in order to do so correctly. Vaccine science has expanded the number of vaccines because vaccine researchers have put in the work necessary to put these vaccines together and get them approved through the appropriate clinical trials.
Allegation – the vaccine companies spent too little time doing the randomized controlled trials.
The issue with this assertion is that the lawyer who said it has no concept of the amount of work required to bring a vaccine idea to reality and set up the RCT. In a pandemic, the trial designers have to strike a balance between logistics, affordability, ability to enroll patients, and when it might be necessary to end the trial earlier than planned and start giving out the vaccine. Even a massive company like Pfizer needs to contemplate how much they can spend on a trial. The attorney’s statements are most strongly refuted by the presence of multiple studies from multiple countries attesting to safety monitoring and effectiveness over the years. You don’t need to rely on only one company to do a trial, especially when you don’t trust them anyway. In addition, all the post marketing trials to check safety within the US were done according to prior specifications. Siri just likes to de-emphasize this. They make the same complaint about the hepatitis B vaccine but then complain there was no placebo. If Siri had dived into the first hepatitis B vaccine documentation, he would have discovered the placebo-controlled trial. When new vaccine updates are available beyond the first generation, it is no longer ethical to give patients a neutral placebo because you are depriving them of protection. The same exercise in literature searching can be used to discover the original placebo-controlled trials of all our major vaccines. The related allegation that certain vaccines were only monitored for a few days is most strongly refuted by a simple literature search demonstrating the sometimes decades of research into vaccine safety monitoring for both the initial vaccine and its subsequent improvements.
Allegation – [in reference to determination of causality of deaths after vaccine], A statistical comparison was conducted when the data supported the desired conclusion but a subjective assessment [was conducted] when it didn’t.
The first thing that ideally should happen is for Aaron Siri to use a bit of introspection and think a little about why this statement does not apply to him. Public health agencies at the national level actually care quite a lot about deaths reported after vaccination. The cause of death is not determined by a swing of a pen, it is determined by a thoughtful discussion by the physician who found the death and detailed review of the medical record. There is a separate statistical comparison of deaths in the placebo versus deaths in the experimental group, but this assessment is meant to figure out if things are occurring more often than expected due to random chance. Both assessment complement each other. The real life analogy is: Do you assume all car crashes are caused by the same reason? You might if you are anti-car and want to spread car fear.
Allegation – Peter Mccullough is one of the most published [researcher on COVID].
While he does have an extensive publication record, he is a cardiologist like me and not trained in infectious disease. His prior publications mostly deal with cardiology before he became an antivaccine advocate. His publication record is also exceeded by Eugene Braunwald, so Mccullough is not the most published cardiologist OR the most published COVID researcher.
Allegation – rapid cardiac death after heart attacks isn’t a thing, but it is with COVID vaccine myocarditis.
Even the sources that Mccullough cites in his testimony, attest to severe myocarditis being a very rare issue. Mccullough is a cardiologist and yet he fails to recall really basic statistics about heart attacks that even students of cardiology know – unfortunately plenty of people die of heart attacks, some even before reaching the hospital. To say that other heart problems don’t cause death within the first eight hours is just objectively false. While vaccine death is correctly assessed as being in the peer reviewed literature, Mccullough lied when he intentionally didn’t say that this was an exceedingly rare outcome made rarer but the lack of systematic autopsy findings that would help search for alternative reasons.
Allegation – there were 216 COVID vaccine deaths in 2025.
It is just a plain old lie to say there are 216 vaccine deaths “this year alone”, when those deaths were actually due to influenza virus.
Allegation – clotting issues affect what we are seeing in the vaccine injured and long COVID.
I think Dr Jordan Vaughn and Dr Josh Greene should be credited to having the most factually accurate testimonies – remember even if you are a Senator, if you don’t have medical training, you may not have the ability to fact check your witnesses in real time. While it is good of Dr Vaughn to provide much needed logic towards his views on COVID clotting, he left out the big elephant in the room which is that COVID vaccination decreases the risk of clot in every epidemiological study that has looked into this.
Allegation – all vials of the vaccine are not the same.
Every public health organization from Australia to the US to Europe has the ability to periodically sample vaccines to make sure there are no significant variability issues. While some studies have found variation in stability, the cold chain storage required for mRNA vaccines effectively preserves them for the company advertised shelf life.
Allegation – [physicians who speak out are exposed to] threats to their medical licenses and board certifications.
It is fundamentally a sign of cognitive dissonance to require peer review for everybody else but exempt yourself from peer review. The obstetrician who discussed this was shown multiple times that his assertions were wrong, but he still equates this with censorship and a threat to his certification. Peer review is fundamentally all about finding logical mistakes and errors, but most of the witnesses cannot stand criticism directed at them. Mccullough’s board certification was removed for a reason that was clearly delineated when he earned that certification – a physician may not willingly give out false or inaccurate medical information. This is a normal standard that all physicians must uphold.
Allegation – “independent researchers with no financial conflicts of interest”
If Peter Mccullough draws more people away from the mainstream narrative his company makes more money. It’s like clockwork – antivaxxers dispute other people’s conflicts of interest but never their own.
Allegation – “[the vaccines] induce fibrin resistant to breakdown”
A great deep dive into why the COVID vaccines are not “clot shots” is here https://deplatformdisease.substack.com/p/are-covid-vaccines-clot-shots?r=nh4jo&utm_medium=ios&triedRedirect=true .
Allegation – “neurological events are the most common side effect after the vaccine”.
This exhibits a failure to simply count. The most common side effects after COVID vaccines are sore shoulders, fatigue, and cold symptoms, same as any other vaccine. While I don’t wish transverse myelitis upon anyone, the frequency of that side effect is less than two per million. I sincerely want Dr Wallskog to get better but this is not an accurate statistical assessment.
Allegation – “3 million lives saved due to COVID vaccines came from a blog”.
While the lawyer who made this allegation wants to make it sound like epidemiological modeling is a technique invented by a kid in a basement, this is actually a subspecialty of epidemiology and borne out by several other professional organizations who have attempted to model the amount of lives saved. The 3 million figure is supported by multiple other sources including direct vaccinated versus unvaccinated comparators which used real life data.
Allegation – “we had an increase in all cause mortality”
The speaker here is trying to paint COVID vaccines as a cause of all cause mortality (ACM). However, he never spent any time thoughtfully reading data we already have available that most of the ACM is generated from the direct and indirect effects of the COVID pandemic such as delayed diagnosis of heart conditions. Vaccine myocarditis is not equivalent to “every medical condition of all causes”.
Allegation – “the COVID vaccine hijacks the cell”
This is a deliberately inflammatory choice of words that forgets that all viruses that infect the human body “hijack cells”. The group of people who embrace this belief also believe you should not wear masks to protect yourself against viruses – so I say the cognitive dissonance is strong.
Allegation – “mRNA vaccine was designed to be unassailable by the body to be broken down”.
This was necessary because externally delivered RNA is notoriously fragile in the human body and rapidly chopped up by the body’s defense mechanisms. It would never survive for any useful medical objective in its usual state. This is a combination of words chosen to be emotionally memorable but scientifically inaccurate.
Allegation – “the spike protein is found all over the body”.
This comes from initial misinterpretations of biodistribution data that were made from Japanese studies involved in assessing COVID vaccines prior to their licensing in Japan. The first mistake is forgetting that less than 1% of the injected vaccine arrives in the other organs, and likely only one component of the vaccine. Some parts of the vaccine were always going to move to lymph nodes because that’s where the immune system processes foreign objects and trains the immune system. Because biochemical history tells us that animal models might need higher doses of things to tell us how specific medicines biodistribute, the mice in the study were given a dose far higher than what a human would ever receive, just so they could detect the signal of the vaccine components. Most people would not take 18-35 times the usual COVID vaccine dose all at once, but indeed at least one guy has done it without any obvious long term effects. Those same biodistribution studies indicate that this vaccine is mostly disposed of in the liver. In addition, prior immunology studies from live attenuated viral vaccines teach us that vaccine antigen circulation after vaccine administration also occurs with live attenuated viral vaccines. While some studies report the presence of spike for months after the vaccination, they are limited by their lack of differentiating between vaccine and viral spike protein, which are structurally different on purpose to prevent vaccine spike from triggering the chemical reactions that the real virus can trigger. While I am happy to be enlightened in the future by studies showing individual variability in immune system processing that can cause things like the hypothesized long COVID after vaccination, it’s wrong to generalize that prolonged spike in many organs is getting people ill like the conference speakers assert.
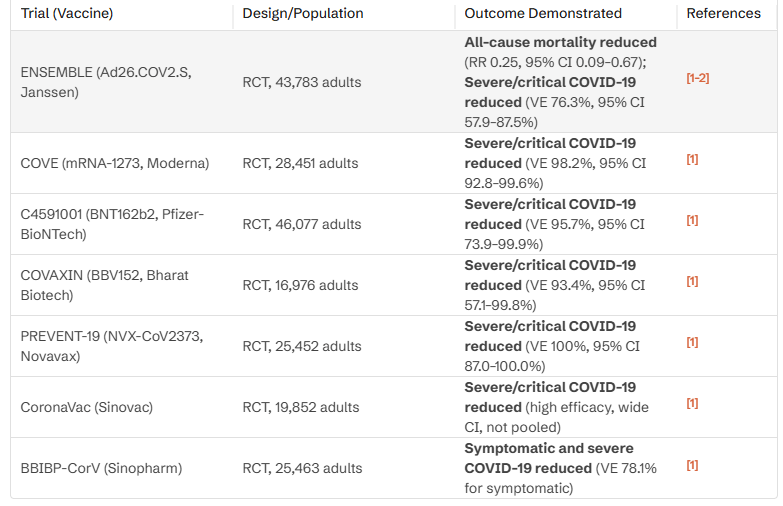
Allegation – There’s never been a prospective randomized double blind placebo controlled trial showing that COVID vaccines reduce mortality or hospitalization.
Watching a former cardiologist lie under oath is especially upsetting because it means both that being under oath doesn’t mean anything anymore, and it means that Mccullough’s morals are such that he doesn’t care if he lies as long as people think he seems credible. There are quite a few trials that show the reduction in mortality or hospitalization with citations following:
https://pubmed.ncbi.nlm.nih.gov/36473651
https://pubmed.ncbi.nlm.nih.gov/35061702
Allegation – “Later COVID mutations were intrinsically more mild”
This is falsified by several studies including this one and the most recent news out of China indicating another COVID outbreak that is causing more hospitalizations.
Allegation – “They lied to us about COVID vaccines blocking transmission”
Different vaccines will reduce transmission to different degrees and COVID vaccines were very effective in reducing transmission in early COVID variants. Later COVID variants were less effectively blocked by vaccination but protection against severe disease remained. While it is justified to be frustrated that politicians didn’t correctly describe this part of vaccines, it is false to say that the physicians / epidemiologists got this wrong. The ability of COVID vaccines to block transmission was spoken about in nuanced terms many times by infectious disease professionals.
Allegation – “statistically zero kids under 5 died of COVID”
Bashing pediatrics is a common theme from many of the antivax testifiers. While not many kids actually died of COVID in the first few years of the pandemic, those kids mattered. They had lives and families and friends who were left behind. This also ignores that far more kids were hospitalized for COVID and needing varying degrees of breathing support. Adult diseases always cause more death and morbidity than their corresponding pediatric counterparts, but to make this comparison superficially and not understand this caveat is intrinsically dishonest. This statement also leaves out the opposite problem, which is the large number of kids who lost parents or were orphaned due to COVID killing their parents.
Allegation – “it was a bad idea to close schools”
Schools cannot be required to stay open in the seasons of highest viral transmission without school leadership and political leadership demonstrating unified financial and resource support to keep those schools safe and the staff members healthy. Debating how to close schools for the next pandemic is absolutely a legitimate debate. However, many in the audience lament the school closures and never actually put up the resources or plans to keep those schools open safely. That’s what makes Senator Moreno’s comments dishonest. If kids are getting sick and going to the hospital, they are not leading productive student lives. Contrary to Senator Morenos claims, kids did in fact bring COVID home to elderly and more medically complex caregivers and got them sick enough to be hospitalized.
Allegation – “we’ve seen long white blood clots in autopsy”
This is derived from the now relatively viral pictures of clots obtained after autopsy. The way these people painted the clots is as “a surprise finding after vaccination”. The issue is all dead bodies have clotted blood. COVID is also well documented to cause blood clots especially in the severely ill. This is what happens when senators try to surprise people without the correct medical context.
Allegation – “ventilators are the worst thing you could have done to people”
Dr Vaughn here is way out in left field. First off, COVID is both a vascular disease and a pulmonary disease; it affects the lungs and the blood vessels. He theoretically completed an intensive care rotation just like myself, and should theoretically know the reasons to put a breathing tube in a patient. While the isolated instances of early prophylactic intubation are debatable in their necessity, the vast majority of intubations during the worst years of COVID were because the patient was going to die without this option. This panel won’t want people to remember, but there were actually people who refused intubation due to fearmongering and then died. COVID requiring ICU hospitalization already has very high mortality, but fearmongering about intubation was especially egregious. While the side effects of intubation were discussed, they were entirely placed out of the correct context.
Allegation – “they should have designed the vaccine against SARS-COV2 nucleoprotein”
One of the recurring themes of this presentation is that vaccine spike protein induces clot. While it is plausible in a limited segment of the population, the studies cited throughout this presentation don’t differentiate between COVID vaccine spike and COVID disease spike. Their logical arguments are much weaker when they fail to accurately distinguish that multiple clinical and laboratory studies prove that COVID viral spike induces clot a lot more efficiently than does the vaccine spike. Designing a vaccine against N protein would weaken the body’s ability to fight off the spike’s ability to generate clot. Secondarily, designing a vaccine against N protein would weaken the body’s ability to neutralize viral particles as antibodies would not stick to the spike protein (which is the primary key of the virus to cell entry). You can’t simultaneously complain about COVID vaccines not sufficiently blocking infection, while advocating for a vaccine that blocks infection even worse. The worst issue with vaccinating against N protein is that we have significant data that suggests such a vaccine might make SARS-COV2 worse, which is something the key speakers in this conference have consistently advocated against. Cognitive dissonance is not their strong suit.
Allegation – COVID vaccine inserts were intentionally left blank
Vaccine companies have told end users many times that the inserts are blank because the most up to date versions are on their corresponding websites.
Allegation – it was reckless to not provide advice on how to decrease the risk of cardiac arrest
By the time a person is receiving a diagnosis of vaccine myocarditis, that person is in front of a pediatric cardiologist or adult cardiologist. This advice comes standard in a myocarditis visit. It is inherently dishonest of Dr Mccullough to insist on the regulators providing this information when it is the role of the treating physician. The CDC has plenty of webpage space already devoted to myocarditis already, as does the European EMA.
Allegation – there is a larger group of subclinical myocarditis
If Mccullough were being honest here he would be equally concerned about subclinical viral myocarditis as well as vaccine myocarditis. Unfortunately, he creates the impression that viral myocarditis is not as serious as vaccine myocarditis, which is false information. The point here is that he is worried that people with subclinical myocarditis are going to get cardiac arrest. He has not done the epidemiological study to show his assertion is right, which makes this allegation entirely personal opinion. We already have studies to show that entirely asymptomatic people don’t have to worry about vaccine myocarditis. In the same segment of this hearing Mccullough is actually describing symptoms of postural orthostatic tachycardia, which although is something that can feel terrible to the patient experiencing it, does not result in heart failure or myocarditis. POTS has occurred after the COVID vaccine but as is true with the other side effects, is a rare occurrence.
Allegation – a study has shown micro scars years after COVID vaccine
He is referring to the study shown here. It is plausible that scars sometimes occur after COVID vaccines, which is again a rare event, but there is epidemiology showing that COVID the disease causes more heart rhythm problems than the vaccine. It is correct to want data on the scar, but it is no longer accurate when Mccullough puts something like this out of context.
Allegation – Vsafe was intentionally designed to not capture adverse events of special interest
Vsafe was designed to quickly capture common symptoms after vaccination and allow end users to quickly report that data to the CDC. The other vaccine monitoring systems have already assessed the cardiac side effects of the COVID vaccine.
Allegation – The Wellness Company has a valuation of 50 million dollars, but pharma valuation is in the billions
While it is not intrinsically an offense to want a successful business, it is problematic to want to push your medications on the public when you have minimal clinical studies to show that it works and ask your customers to take you at your word. I cannot find any clinical research that demonstrates that TWC medications are any better than doing nothing. The dishonesty lies in Mccullough continually wanting better studies from “big pharma”, but not applying that standard to himself. His company has attempted to take advantage of a train derailment in the absence of evidence that it may help those affected by chemical exposure. Any company purporting to make medical products intended to improve health in some way should attempt to back up their claims with something better than personal opinion. Lab experiments have always been designed to give ideas to clinicians to try things, but lab experiments fail in real life for many, many reasons. Mccullough failed to give any clinical evidence in real humans showing his medications work (and why cheaper alternatives don’t work) beyond his personal opinion. We don’t know if his special dandelion and bromelain are just placebo effect.
Allegation – we have an explosion of chronic disease related to immune dysregulation and we need to find the root cause
This is classic antivax maneuvering to make people think that scientists who actually specialize in chronic disease in kids don’t know what they are doing. The most politically effective strategy would be to identify the social determinants of health that are not being addressed in individual communities and fix those determinants. For example, a poor family in rural Wisconsin will not necessarily be able to easily access fruits and whole grains because their local store doesn’t carry it, and they might have to drive all the way into Madison WI to get their food. If they can’t drive because they don’t have public transportation or a car, it either becomes a considerable time expense to get healthy food, or they don’t do it at all. There is no amount of posturing in a Senate hearing that will actually get this problem fixed. Another unaddressed social determinant of health is, if a community doesn’t know how to exercise with the limited resources they have or has safety issues accessing their local park or basketball court, they won’t do it.
Obesity, fatty liver disease, and asthma are three big chronic diseases affecting kids in America today. Each of these diseases has multiple causes, but something that would help immensely is to bring exercise and healthy food into underserved communities affordably. The major molecular pathways of asthma are already laid out if Mr Siri cares to listen, but it is clear that he wishes to paint vaccines as the cause (they aren’t, as per the CHOP vaccine center). Antivaxxers have shown by their track record that if a study produces something they don’t want to hear, they will just criticize vaccines from another perspective. Siri has no sincere desire to find out if asthma is or is not caused by vaccines. Asthma also has multiple environmental causes such as pollution, which the current administration plans to loosen the rules on (again cognitive dissonance is not a strong suit of most of the people testifying today).
Conclusion:
I personally feel no need to encourage people to get COVID vaccines who staunchly don’t want them, but there are still people with medical problems that make COVID infections higher risk. If you don’t want a COVID vaccine, all you need to do is walk away. People who wish to avoid long COVID are also strongly encouraged to be vaccinated at least once.
There is so much good data at this point that nobody should feel the need to lie to get their point across about COVID vaccines. The most charitable interpretation of this conference is that Thorp, Mccullough, Siri, Wallskog, and Vaughn have some fundamental science to remediate – a less charitable interpretation is that they misled people on purpose because they like to promote their preferred point of view. Senator Ron Johnson says he is being accused of ignoring the science – well, most of the points I have made above are facts. A minority of my arguments are opinions. Senators are obligated to get the basic facts right when talking about scientific concepts.
I too want people with vaccine side effects to recover. That salvation isn’t coming from Mccullough, Thorp, Siri, or any of their friends. It will come from people who remain dedicated to the fundamentals of scientific investigation. Ron Johnson wants [science in general] to be painted as corrupt, which then opens an opportunity for all the grifters with their evidence free “cures” to jump into the gap in knowledge. History tells us again and again that this approach ends in disaster. Logical thinking should always prevail.

Leave a comment