This book, released in 2025, purports to share all major scientific failures at assessing vaccine safety and provides the evidence behind its major claims. However, it is very important to understand the premise of the book to get at why the book makes many of the errors it preaches the reader to not commit. The most important conflict of interest is to look into the background of the author – he is the chief lawyer working for the Informed Consent Action Network, one of the largest antivaccine organizations in the United States. It is going to be their mandate to find error in every possible corner of vaccine research to maintain their brand and earn income on more vaccine related lawsuits. If they were to find that a vaccine suited their standards, they would have one less vaccine to file a lawsuit about. Secondarily, the biggest logical error this book commits is the error of false premises. This is when somebody tries to argue with you based upon a statement that is patently false. A more real-world example of this is, “based upon the premise that all airplanes are spraying toxic chemicals into the sky, why won’t you stop all the chemtrails”? This particular delusion arises from believing that all airplane exhaust (a normal expected finding with a plane) is some kind of toxic chemical, whether it be a pesticide, mind control molecule, or whatever. The starting premise is patently false because planes come in all shapes and sizes and serve many different functions, of which only ONE is to spray pesticides. This is the most commonly employed debate tactic or logical error in this book. With that, let’s begin. I’ve included a table of contents because like my other posts, this is not meant to be read in one sitting but used as something like a reference guide. Duplicate arguments are generally omitted. Press the home key to come back up top after selecting the paragraph(s) you like.
Table of Contents
- Introduction
- Chapter 1
- What Stanley Plotkin says is true just because he said it
- Plotkin’s financial conflicts of interest
- Marcia Angell’s opinion on conflicts of interest in the NEJM
- Even Plotkin agrees that placebo controlled RCTs are necessary
- Hepatitis B vaccines were only monitored for five days
- Informed Consent Action Network sends FOIA against the government
- Vaccinologists assert that vaccines cause no harm in the absence of evidence
- MMR has been extensively studied for its lack of links to autism, but the other vaccines have not
- immune dysregulation vs immune priming
- Chapter 2
- It was sanitation that decreased vaccine preventable diseases, not vaccines
- Vaccinologists never infer a vaccine causes harm
- Greg Poland and tinnitus
- Quote: this should have demanded the most impartial committee possible to evaluate whether they should be injected universally into every baby numerous times in the first few months of life
- Chapter 3
- Chapter 4
- Chapter 5
- Chapter 6
- Chapter 7
- Allegation: it is false that measles resulted in 530217 deaths, people stopped dying of measles before the measles vaccine was invented
- Catching measles causes less chronic disease
- Catching measles reduces cancer
- Measles vaccine immunity wanes too much, compared to measles infection
- Diphteria toxin is countered by iron, vitamin C, vitamin B3
- Allegation: they would have kept scarlet fever vaccines if they could, but the amount of scarlet fever out there is now too low to justify a vaccine
- DTP vaccines increase infant deaths by 10 times
- ICANN Lawsuit against UNICEF in 2018
- Allegation: All cause deaths for covid didn’t go down, so the COVID vaccine didn’t work
- Selective application of statistical significance in Pfizer initial trial
- Base rate fallacy with Scottish deaths
- Chapter 8
- Chapter 9
- Chapter 10
- A lack of rationale on why the hepatitis B vaccine is recombinant
- Allegation – no vaccine was tested against a placebo
- Allegation: higher length of monitoring may cause more adverse events
- Influenza vaccine changes each year
- The hepatitis A vaccines had no control group
- Chicken pox vaccine (Varivax) used as part of its placebo control, neomycin
- MMRII was not tested against first MMR vaccine
- Priorix side effects buried
- Allegation – HPV vaccine safety could not actually be evaluated because it was compared to its inactive ingredients
- Big pharma judges vaccine injuries
- Peter Doshi believes the true efficacy of the COVID vaccine was lower
- Chapter 11
- Vaccines cause too many chronic health conditions in kids
- Vaccines cause immune dysregulation
- Pertussis vaccines cause autism
- Aluminium adjuvants cause autism
- IL6/ microglial activation causes autism
- The IOM located sufficient studies to support that 6 serious injuries are causally related to these vaccines
- Allegation – the CDC does not follow its own guidance on how to publish a vaccine safety study
- fewer than 1% of vaccine adverse events are reported
- Allegation: The CDC is ignoring their own propensity reporting ratios when deciding on which side effects are vaccine related
- VSD not reproducible because it is not available
- Vsafe lawsuit
- Henry Ford autism study
Quote: “in the US, the group who is most likely to purposefully choose to not vaccinate are highly educated. In speaking with them, these are people who have read the primary literature themselves, and they’re correctly interpreting it, so it’s not a misunderstanding”
While there are people who are highly educated who decline vaccines, the majority of people who decline vaccines do not have a strong understanding of vaccine science, infectious disease, or epidemiology (see here and here). With some of the major vaccine rumors circulating on the internet, people need to routinely corrected about how vaccines cannot make you magnetic. Other people need to be reminded about how viruses are different from bacteria. Others need to be reminded that hepatitis B is not curable with current technology. Others need to be reminded that we have specific fertility data saying that COVID vaccines have not contributed to a decline in fertility. The mistakes are very extensive and at times, propagated by people with malicious intentions.
Quote: “Then there is what I call the “Vaccines Amen” crowd. This is the group of parents, doctors, and public health professionals I have dealt with—a small army of them—who have a fervent belief in vaccines. This group is often impervious to reason or data”
While Siri correctly criticizes physicians for sometimes just repeating what is said to them, he also fails to acknowledge all the times vaccine researchers have shut down vaccine projects because they had too many side effects or had reasons that caused them to fail. An Australian COVID vaccine project was shut down because it would cause false positive HIV tests. A cancer vaccine for skin cancer failed due to regulatory barriers. Several Ebola vaccines have failed. Siri even discussed the only available Dengue vaccine, that had its indications restricted because it would make Dengue worse in people who never had it before. None of these things would happen if physicians were robots repeating what other people said to them. A more accurate rewrite of this book sentence is that scientists are impervious to the type of reasoning Aaron Siri wants them to have.
Quote: “My personal ideological position regarding vaccines is that vaccines should not be mandated. Everyone should be able to get a vaccine, any vaccine, and get as many as they want. But civil and individual rights demand that no one should be coerced into receiving an unwanted medical product or procedure, including a vaccine.”
This logic fails on several fronts. The most straightforward analogy is through laws. We have laws to prevent various kinds of undesirable behavior, such as traffic rules and seatbelt laws. A highway with absolutely no laws and police enforcement would be considerably more dangerous than a highway with enforced traffic laws. The list of times antivaccine families got other people ill is very long, ranging from the Disney measles outbreak of 2014-2015, the Texas measles outbreak in 2025, and the California whooping cough outbreak of 2010 amongst many others. Informed consent is always available, but the kind proposed in this book is misinformed consent based upon poor understanding of the vaccines themselves. The only real exemptions to vaccines should be medical exemptions.
Chapter 1 The vaccine clergy
Quote: Someone whose claims regarding vaccines are treated as fact based on nothing more than utterance from his lips. The world’s leading vaccinologist, often referred to as the godfather of vaccinology: Dr. Stanley Plotkin.
Dr Plotkin did not just “become a godfather”, he got his start as a new physician and vaccine scientist. He was instrumental as one of the key researchers in the early rubella vaccines, and earned his reputation through consistent hard work in infectious disease and vaccine design. Anyone wishing to prove Plotkin’s scientific experiments incorrect may do so by also using the scientific method. Siri is trained in law, and was out to make Plotkin look as bad as possible, as lawyers are trained to do during deposition. The admittance fee to a scientific debate is the consistent and accurate usage of the scientific method.
Quote: Dr. Plotkin’s long line of incestuous conflicts with the pharma companies that profit from vaccines, including Merck, Pfizer, Sanofi, and GlaxoSmithKline (GSK). These are the same four companies that sell and profit from nearly every vaccine on the CDC’s childhood schedule.
Similar to academic institutions, pharmaceutical companies will want to hire and compensate staff members who have the medical knowledge that they require to develop products that sell. Pharma cannot just hire any bloke off the street. Should Siri be truly interested in decreasing financial conflicts of interest, he should propose members that even the “provaccine team” can agree with. Siri’s law firm would also not hire any old law clerk, they will want people with experience. There are a great many hoops that academic-industry crossover physicians must take to make sure their conflicts of interest are minimized.
Marcia Angell quote for conflicts of interest
The quote being referenced was taken from her statements in the New England Journal of Medicine. Dr Angell does accurately assess many of the limitations of industry funded studies – here Siri does a good job describing the facts. Siri fails in not describing what the medical community has done in response to Dr Angell. Since her commentary, the Physician Payments Sunshine Act has required that all payments from pharmaceutical companies to physicians be documented on publicly available data. I will freely admit I took pharma funded pita bread, but will not try to sell the reader a pulmonary valve that the pharmaceutical company produces. The International Committee of Medical Journal Editors has significantly strengthened their conflict of interest policies. Many institutions around the world have banned pharmaceutical gifts even as small as a mass produced pen. The problem has not been solved forever, and will likely require continued vigilance from all parties and reliance on outside observers.
Even Plotkin agrees that placebo controlled RCTs are necessary
It is factually accurate that Dr Plotkin agrees that placebo controlled randomized controlled trials are necessary. However, the question was set up in a way that implies the previous RCTs should have all been done with a saline placebo. As Siri said, it is unethical to run a study where you intentionally expose people to vaccine preventable disease. He also advocates multiple times throughout the book for a vaccinated versus unvaccinated long term large study. This is inappropriate for multiple reasons, but the simplest two reasons are the population that you wish to enroll. Unvaccinated people living in antivaccine families would never agree to a random chance their children would be vaccinated, and vaccinated families would never agree to their kids going unvaccinated. The second reason is the required sample size for statistical significance would be almost impossible, or impossible to reach.
Hepatitis B vaccines were only monitored for five days
This quote is taken off a FDA fact sheet for a certain hepatitis vaccine. The discussion here is meant to sow enough doubt against the hepatitis B vaccine that it can eventually be delayed and taken off the market. There is considerable momentum within the vaccine hesitant community to remove the birth dose of hepatitis B without considering the epidemiology that lead to that decision. There was an era when the hepatitis B vaccination series matched the same series in Europe, but there were still infants catching hepatitis B which led to chronic liver disease and eventually some cancers. Antivaxxers successfully used emotional hooks, convincing mothers that if they were hepatitis B negative their children could never catch hepatitis B – but the epidemiology in this case didn’t lie. Hepatitis B has no cure as of 2025 and the younger a person is infected, the more likely a permanent infection is to occur. Other countries have different frequencies of hepatitis B which may work (in allowing no birth dose) in those countries – but currently we run the risk of backsliding to the pre-1990s with removal of the early infant doses of hepatitis B. The five days statement is taken specifically from the Recombivax trial. While it is correctly quoted, Siri uses his old trick of taking a quote out of its complete scientific context to ragebait the reader. What Siri won’t tell the reader is that these initial smaller clinical trials were specifically targeted for early/ acute reactions, and that five days is a standard time period to catch these reactions (such as anaphylaxis). What Siri also doesn’t thoughtfully assess is the literature already available about very long term adverse events recorded after hepatitis B vaccine. Using all literature taken together, Siri’s assertion is just factually false.
Quote: Following Plotkin’s deposition, we sent a Freedom of Information Act (FOIA) request to the FDA on behalf of the Informed Consent Action Network (ICAN), the non-profit that funded many of the vaccine policy lawsuits discussed in this book. FOIA is the federal law that allows the public to obtain documents from the government.
While most people can agree that the Federal government should be held accountable to voters via FOIA, what the ICAN repeatedly does is to craft carefully worded FOIA documents to set up the federal government to fail on purpose. One example of a FOIA actually sent from ICAN requested “Documents reflecting any documented case of an individual who: (1) never received a COVID-19 vaccine; (2) was infected with COVID-19 once, recovered, and then later became infected again; and (3) transmitted SARS-CoV-2 to another person when reinfected.” The first reason this is abusive is that FOIA is designed to produce prior documents. The second reason is that the CDC is not designed to collect individual patient level data to this level of detail. The third reason is that the ICAN is able to, with the response of “no records exist”, fake outrage to say that the CDC never studied this situation, when in fact, all available epidemiological evidence indicates that both vaccine based immunity and immunity from viral infection are limited in the case of SARS-COV2. An analogy would be to require the US military to provide every document proving humans were visited by aliens, and then fake outrage when the military is not able to provide these documents and assume there is a alien coverup.
Quote: What is deeply concerning is that vaccinologists will assert that a vaccine does not cause a claimed harm without any proof to support that claim. Even if millions of parents claim a vaccine caused a certain harm, Dr. Plotkin and his disciples will assert that vaccines do not cause that harm, even if they have no evidence to support that assertion.
This is a willful misunderstanding of how research into vaccine side effects work. The simplest level of vaccine side effect research is to assess their statistical frequency. If a vaccine causes side effects, it should be visible in assessment of an entire population more frequently than how much it occurs randomly by chance. For example, if you compare two crowds flashing flashlights at you in the dark, you should be able to measure the increase in brightness of one group if they were truly flashing their lights more than the other. If both groups are randomly flashing their lights the same amount, the observer must conclude that on average the flashing lights occur at the same frequency. If someone had a vaccine and also had a car accident, it would be false to claim that vaccines cause car accidents. At one point in the book, he does make a case for mechanistic studies which is actually a helpful technique that can be used to assess side effects. One example is how Guillain Barre can sometimes, albeit extremely rarely, be linked to influenza vaccines via molecular mimicry. However, this technique is limited by lack of controls and assessment of background rates. A legitimate knowledge gap is how to construct the experiment that shows the step by step biochemical mechanism of how one specific individual incurred a side effect, but Siri shows no sincerity in funding this type of scientific research despite his organization, Childrens Health Defense, having funding to do so. One clinically available test for screening for vaccine side effects before vaccination is the allergy test; tools to predict adverse autoimmune reactions prior to vaccination do not exist in the clinic at the current time.
MMR has been extensively studied for its lack of links to autism, but the other vaccines have not
We recently saw a Danish institution produce an excellent study on the effect of aluminium adjuvants on the later diagnosis of various diseases. At the population level, there was no association. I quote, “This nationwide cohort study did not find evidence supporting an increased risk for autoimmune, atopic or allergic, or neurodevelopmental disorders associated with early childhood exposure to aluminum-adsorbed vaccines.” Aluminium adjuvant research is very important because it applies across many vaccines – and thus helps us to determine that this ingredient is not responsible for autism. Research directly from the world of autism researchers indicates to us that the brain changes of autism can be discovered prior to birth, before the receipt of any vaccine. This is consistent with the finding that the vast majority of autism has a genetic cause (nevermind the fact that autism is actually multiple related diseases). Thiomersal has specifically been studied and it does not cause autism (nevermind the fact that it has been removed from most major US vaccines and the total numbers of autism still rise). Prenatal Tdap vaccine has been studied specifically and it is not associated with autism. If the conflicts of interest listed on this article are inadequate, I would encourage the reader to ponder which alternate funding source would be adequate. Finally, the following meta-analysis assesses whether or not the first generation of diphtheria-tetanus vaccines is associated with autism, and it is not. I would encourage the reader to ask themselves, if a blood test were invented in the future that would predict all serious vaccine side effects – would you also just go ahead and take your chances with the disease, even when the disease is uniformly more dangerous than its corresponding vaccine? Food for thought.
Immune dysregulation vs immune priming
This book routinely conflates immune dysregulation with immune priming. A vaccine is indeed meant to drive the immune system to react to a pretend version of a disease. Characterizing this response as evil is dishonest. Causing a whole new autoimmune disease is an entirely different issue, when your immune system makes a mistake and attacks normal parts of the body when it should not. Clearly, autoimmune reactions have been documented after vaccines, so it is not totally ludicrous to have these thoughts. The autoimmune reaction most relevant to a cardiologist after a vaccine is vaccine myocarditis. However, Siri is doing this area of science a serious disservice by conflating abnormal and normal immune reactions. I would be much more interested in what he had to say had he actually put up funding to improve understanding of the extremely rare autoimmune reactions after vaccines.
Chapter 2 The disciples: vaccinologists
Sanitation v vaccines
The assertion that sanitation mainly caused decreases in vaccine preventable diseases is patently false. While sanitation was very important, it was primarily helpful in reducing diseases spread by fecal-oral transmission, like cholera and typhoid. If sanitation were truly responsible for freeing us from vaccine preventable diseases, all VPDs would decline at the same time, which is clearly refuted in the epidemiology.
The next trick that is usually played is to mix up morbidity and mortality. This means that antivaxxers will try to use getting ill from a disease interchangeably with dying from a disease. This is relevant because the chart typically shown to viewers is disease mortality, which is typically pulled from old epidemiological data. Viewing only this type of chart will give the false impression that people already weren’t dying that much. Viewing the charts alongside corresponding charts showing the frequency of disease, shows that each of our major vaccine preventable diseases steadily declined only after introduction of their corresponding vaccines.
Vaccinologists never infer a vaccine causes harm
It has always been the case that diseases of various kinds will pop up after vaccination. For example, heart attacks have always happened and will continue to happen. Because of this, vaccinologists need to use several techniques to distinguish which diseases are related to the vaccine and which are not. The most basic statistical technique is to compare the rate of disease versus a pre-vaccine baseline, such as comparing the amount of seizures before and after. It is with this type of technique that we know about the mildly increased risk of febrile seizures after the MMRV vaccine (measles, mumps, rubella, varicella) compared to the MMR vaccine. We also are aware of the risk of vaccine myocarditis specifically in young men with COVID mRNA vaccination. An old rotavirus vaccine was even pulled off the market due to the risk of intussusception in infants. Another type of technique is the mechanistic study, which in turn can be done several different ways. The risk of febrile seizures after vaccines was discovered to be sometimes due to a genetic condition in many cases, called Dravet syndrome. This is caused by a genetic mutation in a gene responsible for part of the electricity of the brain. There are legitimate knowledge gaps in the genetic susceptibility to vaccine side effects, but we can also use many sources of epidemiological knowledge to assess the overall benefit versus the overall risk. With all these pieces of information, it is false to assert that vaccinologists never criticize their vaccines.
Greg Poland and tinnitus
The most basic requirement of vaccine safety adverse event reporting is an accurate description of what happened. Greg Poland is unique in that he is also a vaccine researcher, who experienced significant tinnitus after receipt of the COVID vaccine. He has expressed frustration at the CDC for only superficially looking into the relationship of tinnitus to COVID vaccines, despite there being a large number of reports of this problem. The CDC decision that tinnitus is not statistically associated to COVID vaccines was not based upon feelings, it was based upon epidemiological assessments such as this. The author then finds that using this approach does leave people “hanging out to dry”, as in they receive no recognition, compensation, or research into why their particular side effect happened (professor Greg Poland included). What should be done? Work on chemical mechanisms. Current hypotheses include autoimmune nerve damage and special types of allergic reactions. Such patients deserve a visit to an ENT phsyician and audiologist to see if symptoms can be treated. Even the most provaccine physicians amongst us can support medical care for those with sincere side effects. This science could be informed by studies such as these. Insisting on accurate epidemiology still stands though – a huge number of COVID vaccine recipients means a proportionally greater number of people with various kinds of side effects. It is still important to say that while some people may have experienced tinnitus, COVID vaccines are not systematically causing tinnitus in the wider population.
Quote: this should have demanded the most impartial committee possible to evaluate whether they should be injected universally into every baby numerous times in the first few months of life.
The committee responsible for deciding on the birth, 2, 4, and 6 month vaccine schedules in the US would have been the ACIP. The composition of the committee before it was remade according to RFK Jr’s specifications was a group of professionals spanning various professions from medicine to immunology to infectious disease, and more. The worst logical error Siri commits in this section of the book is sharing profuse criticism of the ACIP’s conflicts of interests, while making no effort whatsoever to assess how the ACIP has worked over time to decrease its conflicts of interest. The policies on how the ACIP decreases potential COI has been public for a while, as have the individual member disclosures.
Chapter 3 Priests: Medical profession
A grievance on the lack of recognition of natural immunity
The major medically relevant argument in this chapter is frustration over the lack of recognition of immunity derived from infection. While we should study virus derived immunity, the complaints about the lack of recognition of SARS-COV2 derived immunity occurred well before we had specific data to back up these claims. The most severe harm resulting from claims such as these, relevant to COVID, would be hospitalization, death, and long COVID, all of which severely impact people’s lives. Making assertions about natural immunity prior to having studies is inherently unscientific, despite Siri’s constant admonishing the scientific community to be more scientific. Another disease with a famous consequence of virus derived infection is measles – which can cause the immune system to forget every prior infection, as well as cause a very severe type of brain damage resulting in a nearly uniformly fatal death rate if the virus is caught while unvaccinated for measles. None of these consequences of natural infection should be acceptable in the era of vaccines.
Chapter 4: 1986 Vaccine act
Frivolous vaccine lawsuits
The single most significant legal grievance Siri has against vaccine laws is the existence of the 1986 National Childhood Vaccine Injury Act. He believes this shields vaccine companies from liability which then financially removes the incentive to make safer vaccines. While this is a potential superficial interpretation of the act, it misses both the work that is already done as well as the actions of the Informed Consent Action Network and related organizations similar to ICAN. First off, the assumption of this chapter is that there are basically no times when vaccine companies criticized or shut down their own vaccine projects. This is soundly refuted by the long list of vaccine trials that failed along various steps of the way prior to complete FDA approval. Second, frivolous lawsuits are most definitely a problem and the most direct problem the 1986 Act is meant to prevent. The largest example of this is the Autism Omnibus proceedings, where thousands of families took to court to argue the case that their child’s autism was caused by their vaccine. The then relatively new National Vaccine Injury Compensation Program brought all these cases together into a large court proceeding and ultimately ruled that these cases had no factual justification. In another case, a potential Lyme vaccine was destroyed by antivaxxers even in the absence of clinical justification. Again, while even the most pro-vaccine physicians would like for patients to receive treatment and compensation of severe side effects, this book is clearly trying to present only one side of the argument.
Side effects of DTP were too significant
The book devotes a lot of time to decrying the side effects of the DTP vaccine, which are correctly assessed as more frequent than the side effects of the newer DTaP vaccine. However, this section of the chapter drops any mention that vaccine companies eventually recognized the problem and in the US at least, invented the newer DTaP vaccine to help cut down on those side effects. Another example of presenting only the preferred side of the story.
Chapter 5: The public face – regulators
HHS mandated vaccine safety reports every 2 years
The author very simply declined to connect this part of the chapter to all the other safety studies that were released through the HHS or through its affiliates, that looked into vaccine safety over the many decades the CDC/ HHS/ VAERS/ VSD have been assessing vaccine safety. The rest of the book basically refutes this assertion. Not a good look to refute yourself in your own book.
CDC never criticizes its vaccines
The author has missed an entire website on the CDC webpage where they listed deficiencies or criticisms of many different vaccines.
Chapter 6 the real power – pharma
Why vaccines are regulated differently than drugs
The author laments the observation that drugs are monitored for a longer time period than vaccines prior to their release to the general population. The general idea of how a vaccine arrives on the market is as follows:
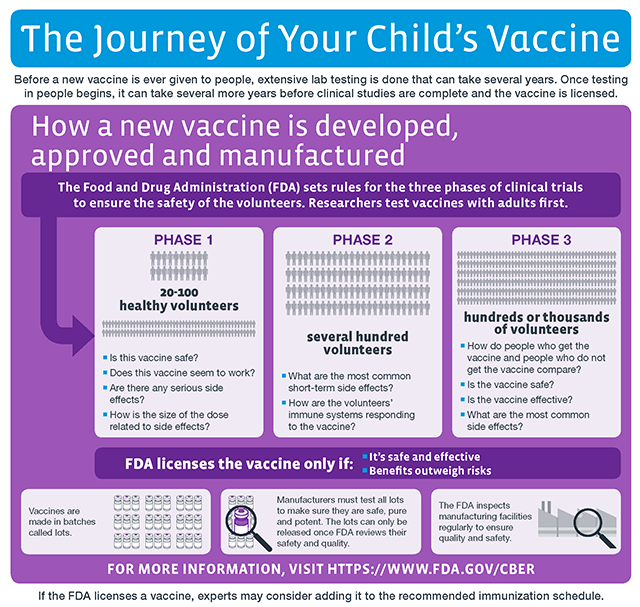
A similar chart for a drug is as follows:
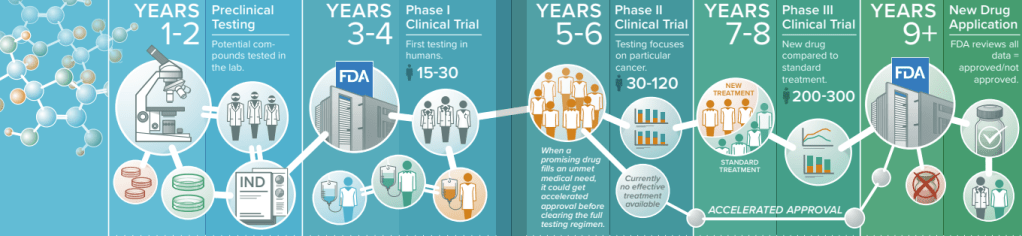
The authors assertion fails to realize that both vaccines and drugs have to go through extensive discovery processes and similar clinical trials in order to get on the FDA’s desk for eventual approval. The Hepatitis B vaccine is described multiple times throughout the book as having only been tested for five days, but this is an intentional misrepresentation that forgets that the trial that monitored the vaccine for five days was specifically looking for immediate allergic reactions ONLY. The five day length would be appropriate for that clinical question, but multiple long term studies are also available for perusal. Both drugs and vaccines are monitored for immediate allergic reactions and both drugs/ vaccines are monitored in the long term. Ultimately, vaccines are monitored by so many different safety monitoring systems that from certain perspectives, they are held to higher standards than drugs.
Project veritas citations
Project Veritas has a long track record of using terrible journalistic practices.
Chapter 7 – vaccines save millions of lives
Allegation: it is false that measles resulted in 530217 deaths, people stopped dying of measles before the measles vaccine was invented
While the 530,217 number is correctly cited, this section of the chapter is incorrectly trying to assert that the vaccine didn’t matter because people were already dying less. The author didn’t learn anything since chapter 2, and here is the reason why. He is mixing up morbidity and mortality. This means that antivaxxers will try to use getting ill from a disease interchangeably with dying from a disease. This is relevant because the chart typically shown to viewers is disease mortality, which is typically pulled from old epidemiological data. Viewing only this type of chart will give the false impression that people already weren’t dying that much. Viewing the charts alongside corresponding charts showing the frequency of disease, shows that each of our major vaccine preventable diseases steadily declined only after introduction of their corresponding vaccines. A secondary refutation is that no amount of handwashing and better sewage will effectively contain an airborne disease, which is measles (you can’t wash your hands, not wear a mask, and expect to be able to avoid measles). A similar assessment can be performed for the DTaP vaccine.
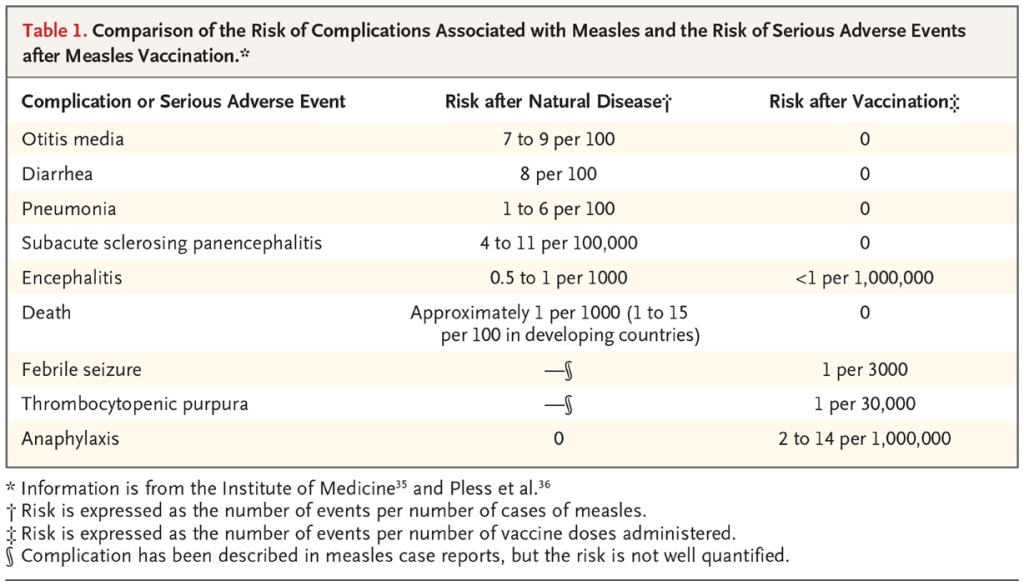
Allegation: Catching measles causes less chronic disease
It is pretty much never appropriate to ask in public health, for the general public to just go catch a disease to get immunity when the potential consequences of severe disease are so great. Furthermore, we have an actual study assessing the side effects of measles versus measles vaccination, specifically assessing some chronic diseases that soundly contradict the claim. The author was never good at reading studies he didn’t want to hear.
Allegation: Catching measles reduces cancer
A review has already been completed soundly refuting this assertion. The most serious debunk of this allegation is that cancer patients are frequently immunocompromised, and a real measles infection would be actually life threatening.
Measles vaccine immunity wanes too much, compared to measles infection
This assessment is guilty of taking facts out of context. It is correctly assessed that measles antibodies have been observed to wane faster with the vaccine than with the illness. One reason is that if your body constantly produced high levels of antibodies against everything, there is an actual disease state that does this called multiple myeloma (and your blood couldn’t function). However, both clinical and modeling studies indicate that recipients of measles vaccines maintain long lasting immunity against severe disease for decades. A blood test and the ability of a whole human with an intact immune system to prevent disease are two different things.
Diphteria toxin is countered by iron, vitamin C, vitamin B3
This assertion comes from taking laboratory studies out of context and forgetting that what is true in the super controlled conditions of a lab, is not necessarily true in a human being. The standard of care remains to take vaccination as the best preventative, use an antitoxin as needed during severe disease, and potentially antibiotics.
Allegation: they would have kept scarlet fever vaccines if they could, but the amount of scarlet fever out there is now too low to justify a vaccine
Group A streptococcus, the causative agent of scarlet fever, is easily treated by antibiotics. This is where a lack of clinical knowledge significantly impairs the discussion on vaccines. If vaccinologists could find a way to design a scarlet fever vaccine following the strict guidelines of all the other vaccines, they absolutely could. Many groups have tried. However, the barriers to designing both a safe and effective vaccine are quite high because of the risk of autoimmunity and the large variety of group A strep bacteria. This also refutes the allegation that vaccinologists could never criticize their own vaccines.
DTP vaccines increase infant deaths by 10 times
This allegation comes from the work by Stabell-Benn and Aaby on the DTP vaccine and measurements of infant mortality in an isolated population. The issue with taking this data at face value is the presence of confounders – this group studied isolated populations with much different healthcare access and much less access to timely diagnosis of conditions that would influence infant mortality. Furthermore, larger population studies refute the assertion, such as these two studies here and here. This is another famous intellectual trick used by antivaxxers – cite lower quality studies and ignore the higher quality studies. While it is accurate that DTP may create more side effects than DTaP, trading the old DTP for the new DTaP has tradeoffs that national public health agencies have to discuss.
ICANN lawsuit to UNICEF in 2018
This lawsuit was based upon false premises discussed in the paragraph above.
Allegation: All cause deaths for covid didn’t go down, so the COVID vaccine didn’t work
This represents a poor understanding of epidemiology. The definition of all cause death is the absolute or percentage of deaths in a population. The reason this statistic is helpful for policymakers is because it can help assess during a viral pandemic, whether or not people are dying from various causes related to the pandemic infection. The primary intent of vaccination is never to reduce all cause deaths from everything under the sun – clearly a vaccine cannot protect against American gun violence, deaths from police brutality, or car accidents. COVID vaccinations can be relied upon to protect against some of the excess mortality via decreasing deaths attributable to COVID19, such as blood clots or heart failure. Secondarily they can protect against overwhelming the hospital system. Multiple academic centers have shown that COVID vaccination protects well against COVID related mortality and does not increase mortality from other causes.
Selective application of statistical significance in Pfizer initial trial
This book laments the observation from the Pfizer initial clinical trial for licensing the COVID vaccine, that the amount of deaths in the vaccine group was greater than in the control group. The book author however, conveniently omits the observation that this difference was not statistically significant. To understand the deception requires an understanding of what statistical significance means – it is essentially a mathematical equation that tells you something is highly unlikely to have occurred by chance. If you were to see a UFO once, other people could argue that you saw a projection from a TV screen, a commercial, or something like that. However, if you brought pictures, saw the craft, touched the craft, met the pilots, and shared some bread, it would be highly unlikely that all this occurred by random chance alone. Mathematics can help us do something similar with the difference between two groups. The dishonesty comes when Siri does point out statistically significant comparisons that try to lure the reader into a false argument, such as in the measles chapter. While the mathematics was calculated correctly, fixating on that observation alone requires ignoring the dangers of measles in order to seek out the apparent reduced risk of chronic diseases. This also ignores the chronic diseases that measles itself causes. An honest actor cannot selectively apply statistics only when it is helpful for his arguments.
Base rate fallacy with Scottish deaths
When there is a vaccinated and unvaccinated group to start out with, you can start comparing the deaths in the two groups. Pretty universally, unvaccinated people die more from the vaccine preventable disease being studied. As people interested in vaccines start to get vaccinated, the pool of people staying unvaccinated gets smaller and smaller. At some point, the vaccinated will still periodically get mild disease because vaccines don’t typically stop all mild disease, however they have still done their job of protecting against disease severe enough to require hospitalization. Some unvaccinated will be able to be spared from severe disease, which is great for them, but not a generalizable finding. At some point, the apparent group of vaccinated getting ill with all levels of disease will exceed the number getting ill with all levels of disease, who are unvaccinated, because the pool of unvaccinated patients is so much smaller. However, it would be false to insinuate that the vaccines cause more death while failing to account for the much larger vaccinated group. This is the base rate fallacy.

Chapter 8 – vaccines save millions from harm
ICANN petition for the Polio vaccine
Aaron Siri did file a legal petition against the IPOL polio vaccine. This is a polio vaccine by itself unlike the combination vaccines more commonly used in the US. The idea behind his lawsuit is that he wanted the vaccine to be suspended until a proper randomized controlled trial can be conducted for it. Secondarily they wanted the vaccine label to be edited to say that the vaccine does not do anything for transmission. This sounds like a rational demand until you dig deeper (hint hint, nudge nudge). The lawsuit does correctly assess that a complete randomized RCT versus placebo was not conducted to approve IPOL, based upon a reading of the IPOL label. However, it would be unethical to conduct a randomized controlled trial in 2025 when we already have abundant evidence on the need to protect against poliovirus. Secondarily, it is important to keep a single antigen vaccine available for those who need a polio booster who are unable to get the combination vaccine. Lastly, while it is correct to assess that inactivated poliovirus doesn’t protect against gastrointestinal infection as well as the oral poliovirus vaccine, we already have plenty of data to show that poliovirus is already very effectively suppressed in communities with high immunity from vaccination even in countries that provide the IPV vaccination. The most important goal of polio vaccination is to prevent paralysis, and the IPV vaccination already does that.
Allegation : Polio decrease in cases/ paralysis is an artifact of diagnostic criteria
This is false because of several lines of evidence. First off, multiple countries observed a decrease in polio cases after vaccination. Secondarily, from the same source, polio surveillance systems allowed direct virologic confirmation of cases. Lastly, clinical polio cases mirrored a decline in actual samples of patients showing polio. This again demonstrates the danger of making these types of assertions with a lack of medical knowledge.
Allegation: Kleinman believes the polio vaccine is useless
This section of the book uses the tactic of quoting experts out of context and ignoring the overall scientific consensus. Professor Kleinman was lamenting the lack of efficacy of the very first polio vaccines against certain subtypes of poliovirus (there are three). The most straightforward rebuttal to this assertion is that the modern polio vaccine has strong protection against all three types of poliovirus. The public health staff members being depicted in this part of the chapter were engaging in legitimate debate about the deficiencies of the polio vaccine available at the time, and vaccine science acted on their concerns by changing the number of doses, changing the time of the doses, and inventing newer iterations of polio vaccines to reach the strong polio vaccine coverage we have today.
Chapter 9 – Vaccines prevent transmission
IPV doesn’t prevent transmission of polio
While it is correct to assess that inactivated poliovirus doesn’t protect against gastrointestinal infection as well as the oral poliovirus vaccine, we already have plenty of data to show that poliovirus is already very effectively suppressed in communities with high immunity from vaccination even in countries that provide the IPV vaccination. The most important goal of polio vaccination is to prevent paralysis, and the IPV vaccination already does that.
Pertussis vaccine doesn’t prevent transmission
This is correctly assessed as a limitation of the pertussis vaccine but omits the fact that the most important role of this vaccine, to prevent severe disease, has been achieved.
Tetanus vaccine doesn’t prevent transmission
This bacteria is somewhat unusual in that it is primarily transmitted by punctured skin and dirty metal objects. The primary mechanism of severe disease in tetanus is the toxin’s effect on the body. Therefore, it is not a disease transmitted from human to human. Therefore, a vaccine does not need to prevent transmission to be effective, it needs to help the body delete the tetanus toxin.
MenACWY doesn’t prevent transmission
By now the pattern should be getting familiar – infectious disease physicians do agree that meningitis bacteria do colonize the nose in some people, without creating disease. However, the vaccine still does its job well in preventing severe disease.
Hepatitis B transmission in kids
The allegation here is always that hepatitis B vaccine is only necessary in kids born to mothers with hepatitis B. Infectious disease physicians care deeply about hepatitis B because it has no cure and the younger you catch it, the more likely you are to have permanent liver damage. Children may catch hepatitis B through multiple pathways that are not sex, drugs, and rock and roll. A nonexhaustive list includes the sharing of toothbrushes, accidental cuts in the skin that then rub onto an infected object, and accidental bites from people infected with hepatitis B.
Those who are not vaccinated wish to force their decision on others
The list of times antivaccine families got other people ill is very long, ranging from the Disney measles outbreak of 2014-2015, the Texas measles outbreak in 2025, and the California whooping cough outbreak of 2010 amongst many others. Informed consent is always available, but the kind proposed in this book is misinformed consent based upon poor understanding of the vaccines themselves. Real effective consent is not misinformed. The only real exemptions to vaccines should be medical exemptions. The cancer patient wishing to not be ill from measles doesn’t have a choice when an unvaccinated family actually infected with measles gives that cancer patient the real measles disease.
Chapter 10 – vaccines are studied pre licensure
Lack of rationale on why hepB is recombinant
Siri spends a great deal of time complaining about how the hepatitis B vaccine is a “recombinant vaccine”. He fails to understand the core rationale for this – when you make just the hepatitis B virus surface protein, in a test tube from scratch with the assistance of yeast, you guarantee there is no other protein contamination from the start. The first vaccine for hepatitis B was derived from purification of human blood and had potential for contamination with other allergy generating proteins.
Allegation – no vaccine was tested against a placebo
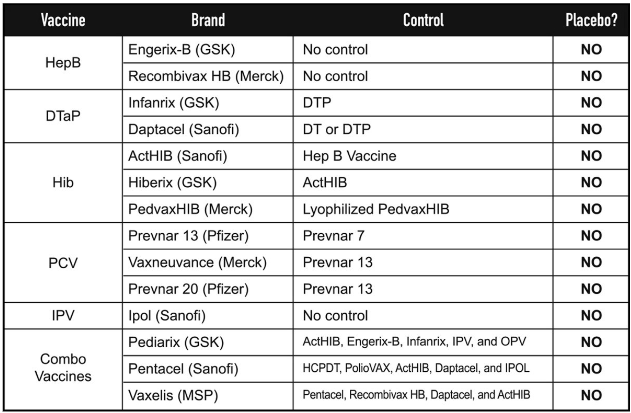
With this table Siri attempts to share with us that all vaccines have no controls. This is false. His logical mistake is not going back to the true first generation of each of the vaccines. For the hepatitis B vaccine that was originally purified from human blood, a placebo comparator was used and is explictly stated to be the inactive ingredient of alum in this particular trial. Several different old pertussis, tetanus, and diphteria vaccines led up to the modern DTaP vaccine. The very first pertussis vaccine was absolutely compared against no vaccine. The combination vaccine was tested in several different formats and is therefore more complicated due to the ethical considerations of withholding diphtheria/ tetanus protection in early iterations of the vaccine, but there are absolutely some combination vaccines that were compared against placebo. The drug label of the original PedvaxHIB vaccine is clearly described as being compared to a placebo with additional DTP/OPV vaccinations. The first pneumococcal vaccine was compared to a meningitis vaccine, but this was done to give all trial participants a similar injection experience. This still means the vaccine’s safety was studied in other ways for many years after initial licensure. For the polio vaccines, again the reader must reference the very first polio vaccines, the Salk and Sabin polio vaccines, to discover their saline/ sugar placebos, and not reference a newer generation of polio vaccine. Lastly, combination vaccines will not be tested against saline placebo because by the time combination vaccines are invented, there are first generation vaccines already licensed for which it would be unethical to test against placebo and randomize to disease exposure.
Allegation: higher length of monitoring may cause more adverse events
This allegation is worded several different ways depending on the antivaccine book that you read. Sometimes, the author states that vaccine companies refuse to monitor the vaccine for prolonged periods of time because it would expose more adverse events. Other times, people say that the longer we look, the more adverse events we find. The issue is the biological plausibility of the adverse events themselves. If you believe as Peter Mccullough does, that every cardiac event after the vaccine is caused by the vaccine, you have to believe that each component of the vaccine has an unlimited shelf life and unlimited life within the body. This is clearly refuted by the ways that the body metabolizes things and turns over old material. Pretty much nothing in the body stays in its original untouched state forever. Many different biological tools are used to determine what a vaccine adverse event is from. For example, immediate severe allergic reactions cannot plausibly occur two years after the vaccine. Another example is the typical time span of vaccine myocarditis 2 days to 2 weeks after a mRNA vaccine. The time lengths recognized in the literature are not selected for fun, they are based upon biological plausibility and known behavior of the components of each vaccine. If the antivax community wishes for mainstream physicians to believe their evidence, they need to raise the quality of their evidence.
Influenza vaccine changes each year
The allegation here is that the influenza vaccine is not adequately tested because the formulation changes every year. One way this question would be permanently resolved is to have a universal influenza vaccine that works on all types of influenza, but alas, this vaccine is in the research stage. The reason the current vaccine for influenza is changed every season is because the virus changes every season. If Siri truly had his way and the new version of the influenza vaccine needed to be completely re-approved by the FDA each season, the approval process would be so slow that the vaccine would only be approved by the time the flu season had already stopped.
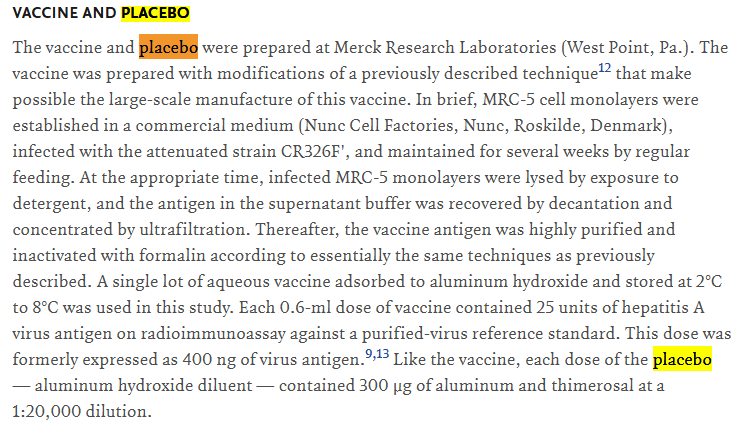
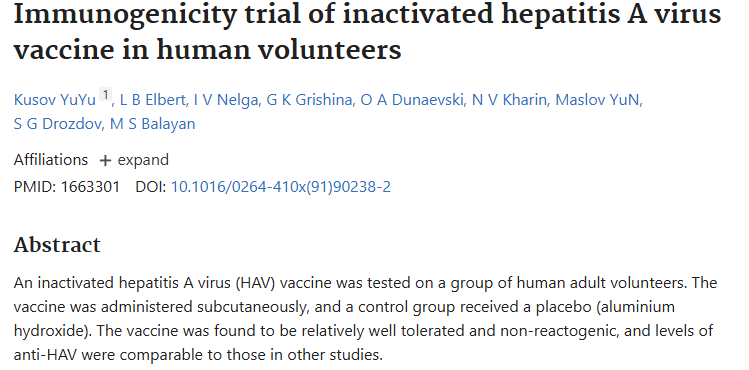
The hepatitis A vaccines had no control group
The initial clinical trials for these vaccines are plainly spelled out as the vaccine adjuvant by itself without active ingredients. This is not debatable.
Chicken pox vaccine (Varivax) used as part of its placebo control, neomycin
While this is correctly cited, the modern Varivax label contains clearly labeled instructions to not use the vaccine if you have an allergy against any of the components of the vaccine. The existence of antibiotic allergy is very well studied and documented. There are not really any doubts on what should happen in a patient with antibiotic allergy.
MMRII was not tested against first MMR vaccine
I doubt the author’s sincerity if he complains both that vaccines were not tested against placebo, but when there are some vaccines available tested against placebo, he complains again. The biggest refutation of this assertion is that one of the most important motivations to invent the next generation MMRII vaccine was to improve on vaccine safety. Next, we already know the frequency of side effects for the MMR vaccine. Lastly, we now have a variety of MMR vaccine clinical trials tested against various types of placebo, including prior monovalent MMR vaccines.
Priorix side effects buried
The author alleges that the manner in which the side effects were brushed aside is by placing them in a supplementary table. First off, the side effects were statistically compared and found to be similar. Next off, we already have statistical comparisons between older MMR vaccines and their placebos showing that the rate of side effects is comparable. No hiding occurred.
Allegation – HPV vaccine safety could not actually be evaluated because it was compared to its inactive ingredients, and HPV vaccines caused autoimmune disorders in some kids
It’s not that hard to find the clinical trial that compared an old HPV vaccine to saline placebo. The highest level of evidence available teaches us that HPV vaccines do not systematically raise the risk of autoimmune disorders.
Big pharma judges vaccine injuries
The allegation here is that pharmaceutical companies get to judge whether or not their vaccines cause side effects and have no accountability. First off, multiple side effect monitoring systems exist in different countries that catch what the initial clinical trial didn’t catch. Next, the systematic approach to determining a vaccine side effect is well established and also carries legitimate critiques on how to improve it. The additional safety monitoring systems also manage to catch side effects which then are shared by national health agencies. Just like other provaccine physicians I can see ways the vaccine side effect monitoring system can be improved, but the oversimplification that vaccine companies get to judge side effects is false.
Peter Doshi believes the true efficacy of the COVID vaccine was lower
This assertion was best debunked here.
Chapter 11 – vaccines are carefully studied post licensure
Vaccines cause too many chronic health conditions in kids
The absolute largest studies in the world soundly refute this claim.
Vaccines cause immune dysregulation
This is usually worded as a complaint that vaccines cause dysregulation of the immune system or autoimmune problems. Again, the largest studies in the world soundly refute this claim. There wasn’t even an attempt to even discuss why the author’s beliefs are contradicted by meta-analyses.
Pertussis vaccines cause autism
Usually when someone who is antivaccine feels like their vaccines/ autism argument is fading, they will resort to the argument that well, the MMR vaccine was tested, but the other vaccines were not tested for autism. Except – the Tdap vaccine given prior to pregnancy has been shown to not raise autism rates.
Aluminium adjuvants cause autism
This has been soundly debunked here.
IL6/ microglial activation causes autism
While the evidence for this as being one of the mechanisms of autism like symptoms, is reasonable, the data do not support consumed aluminium as being the source of the IL-6 activation.
The IOM located sufficient studies to support that 6 serious injuries are causally related to these vaccines, including acute encephalopathy (brain damage) and chronic arthritis. It located sufficient studies to rule out 4 injuries as not related to these vaccines.
The most significant logical error in relying on their report at face value is that the absence of evidence, does not on its own prove the side effects are related. A medical organization making a statement that insufficient evidence exists to link a vaccine to a side effect, in Medical English, means both that the side effect has not been linked, AND that we may not then just casually believe that the side effect is definitely caused by the vaccine. We need to still rely on our safety monitoring systems to catch rare side effects and eventually figure out why they occur.
Allegation – the CDC does not follow its own guidance on how to publish a vaccine safety study
The authors cites the following CDC white paper as evidence that more vaccine side effects are hidden. There are multiple examples of how vaccine safety studies were conducted using the template, one example of which is shown here.
Fewer than 1% of vaccine adverse events are reported
This statement is debunked here.
Allegation: The CDC is ignoring their own propensity reporting ratios when deciding on which side effects are vaccine related
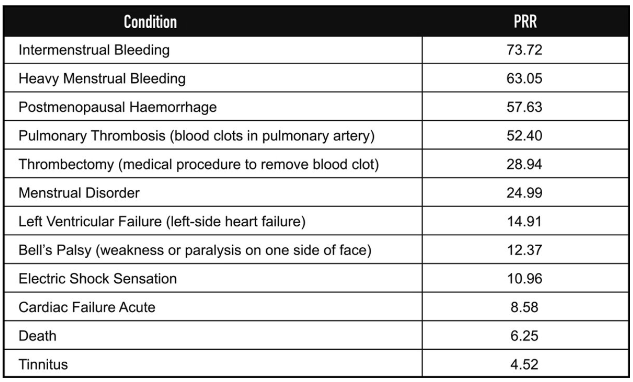
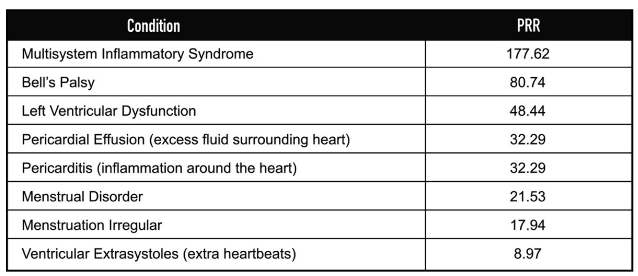
This is a failure to understand the original purpose of calculating the propensity reporting ratio, which is a statistical way to understand how much more common is a particular side effect compared to a previous known baseline. This assertion also ignores the multiple times the CDC/ACIP have changed course after identifying a PRR generated side effect. Next, because the PRR is calculated from passive reporting systems like VAERS, they suffer from both under and overreporting. Lastly, multisystem inflammatory syndrome is clearly established as a COVID disease side effect with a genetic cause . The cardiac side effects of the COVID vaccine versus COVID disease are likewise very well established by this point.
VSD not reproducible because it is not available
This assertion ignores the structure of the VSD. The database is a collaborative project between multiple healthcare organizations who must mutually sign data sharing agreements and research protocols, which effectively decrease the risk of one physician unilaterally altering data. Any researcher wishing to design a protocol using VSD data may discuss their project with prior VSD staff.
Vsafe lawsuit
The reader is reminded that the author and his parent organization/ supporters, are financially compensated by continually churning out lawsuits regardless of their factuality. When a lawsuit wins, it is a feather in their cap regardless of whether or not the lawsuit accomplished anything substantive. While Siri did expend a lot of work trying to expose the entire Vsafe database, his lawsuit did not reveal much in the way of previously unknown data. The interested reader may peruse how medical systems try to balance patient confidentiality with transparency/ third party review here.
Henry Ford autism study
The timing of the book release was timed to coincide with publicity on an autism study conducted in the United States in the Henry Ford health system, however as is the usual pattern here, the book author failed to notice the study’s numerous weaknesses before relying on it as a cornerstone of his argument. The study is addressed in much better detail here by statistician Jeff Morris. Vaccines still don’t cause autism.

Leave a reply to immunie.circuits.modeling Cancel reply